Your health deserves
the ultimate care
Portrait


Philosophy
Experience
Private practice in Geneva
Trainer and international reputation
CV
Complete version of the CV on LinkedIn
- Doctor of Medicine, University of Liège (Belgium), 1998: summa cum laude
- Specialist in Neurosurgery, Universities of Liège and Geneva, 2004
- European Diploma in Neurosurgery, 2004
- European Diploma in Pediatric Neurosurgery, 2007
- USMLE (United States Medical License Examination) step 1, Paris 1996
- USMLE (United States Medical License Examination) step 2, Paris 1997
- ECFMG (English Language Proficiency Test), Geneva 1998
- TOEFL (Test Of English as a Foreign Language), Brussels 1998
- EANS (European Association of Neurosurgical Societies) Complete curriculum 4 years
- ESPN (European Society of Pediatric Neurosurgery) Complete curriculum 4 years
Scientific Awards :
- Rhone-Poulenc Prize 1998: Best results during medical studies
- Laureate of the International Rotary Foundation, 2003
Functions :
- 2013 – present: Neurosurgeon in private practice, Geneva, Switzerland
- 2012: Head teaching physician in Neurosurgery, Belgium
- 2005 – 2012: Neurosurgeon and Pediatric Neurosurgeon, Liège, Belgium
- 2003 – 2005: Chief Resident then Junior Staff Member, University Hospital of Geneva, Geneva, Switzerland
- 1998 – 2003: Resident in Neurosurgery
- University of Liège, Belgium
- University of Geneva, Switzerland
- Harvard Medical School, Boston, USA
Associations :
- Member of the North American Spine Society (NASS)
- Member of the Belgian Society of Neurosurgery
- Member of the Doctor’s Association of Geneva (AMG)
- Member of the Society of Lateral Access Surgery (SOLAS)
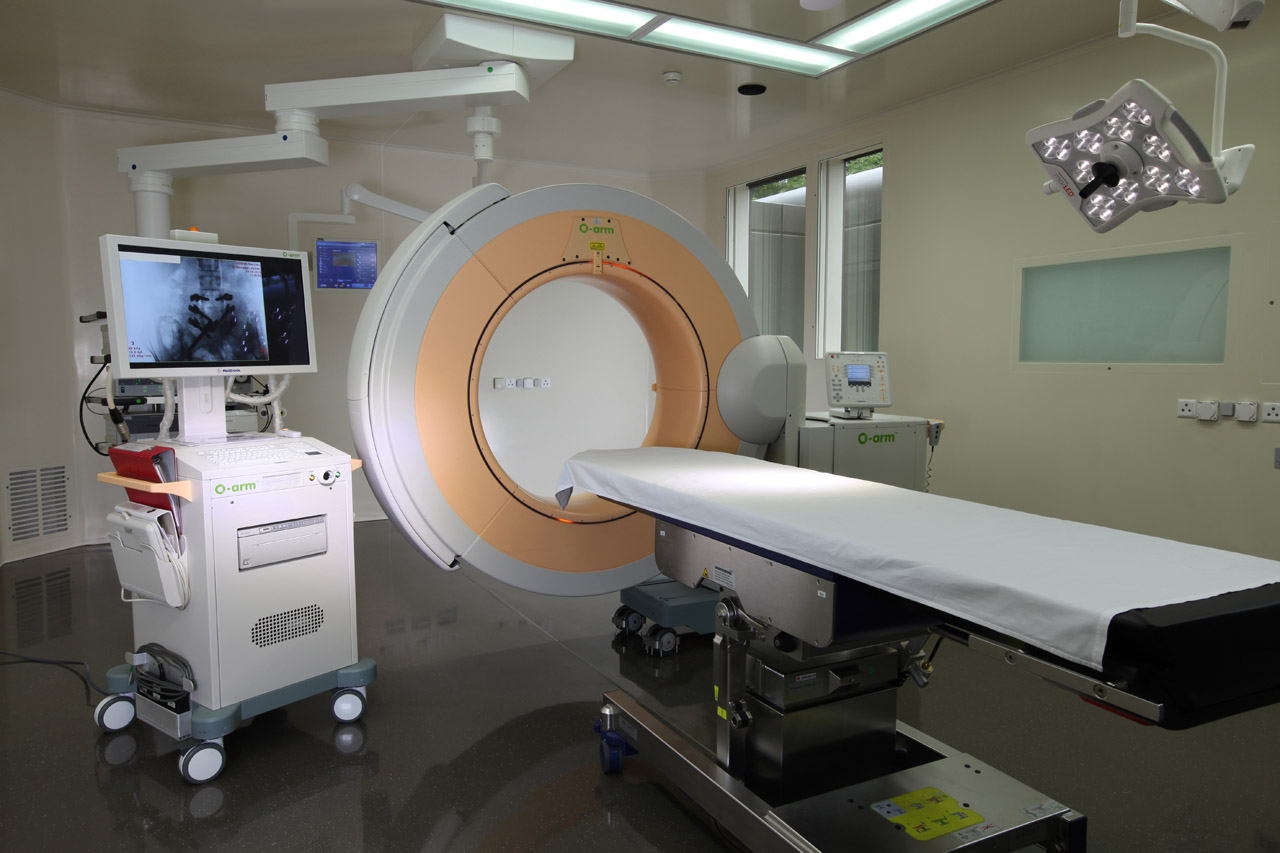
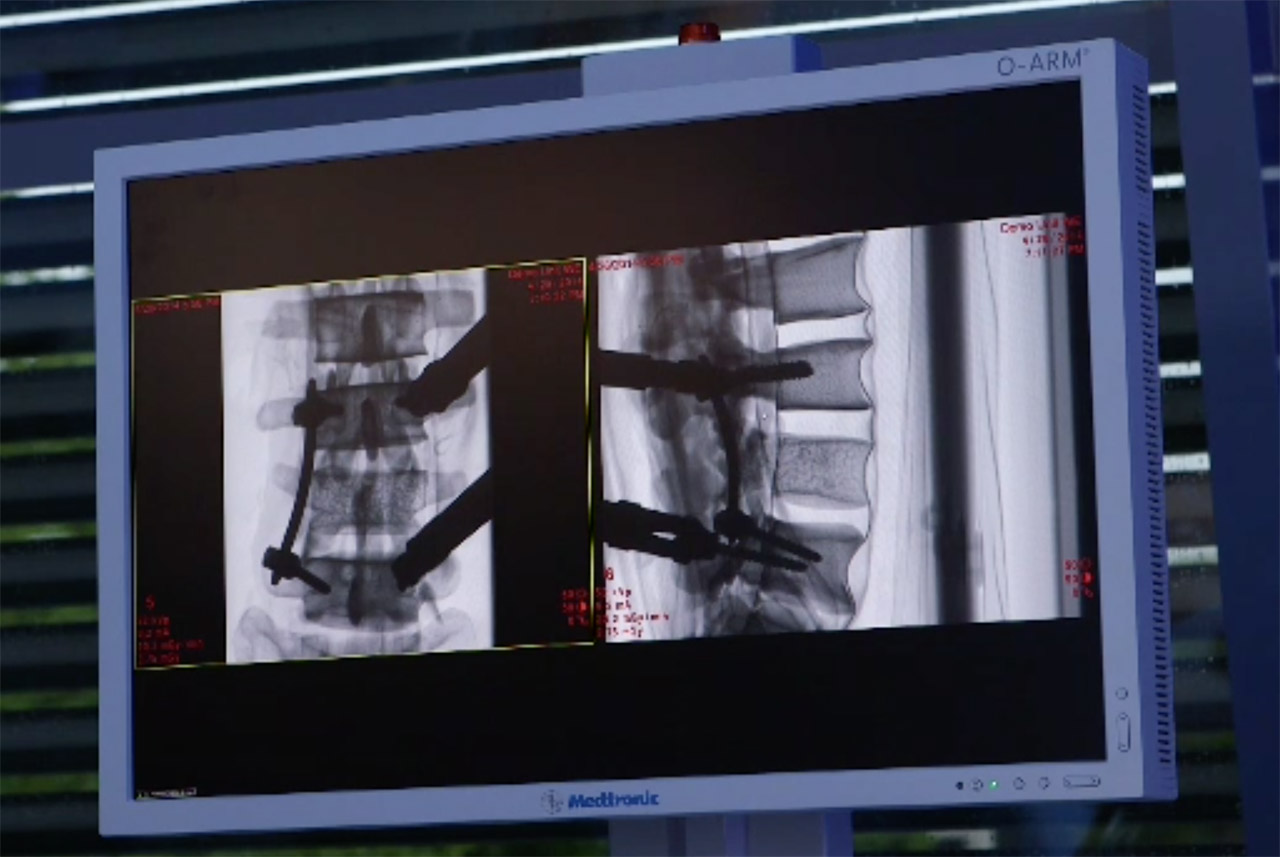
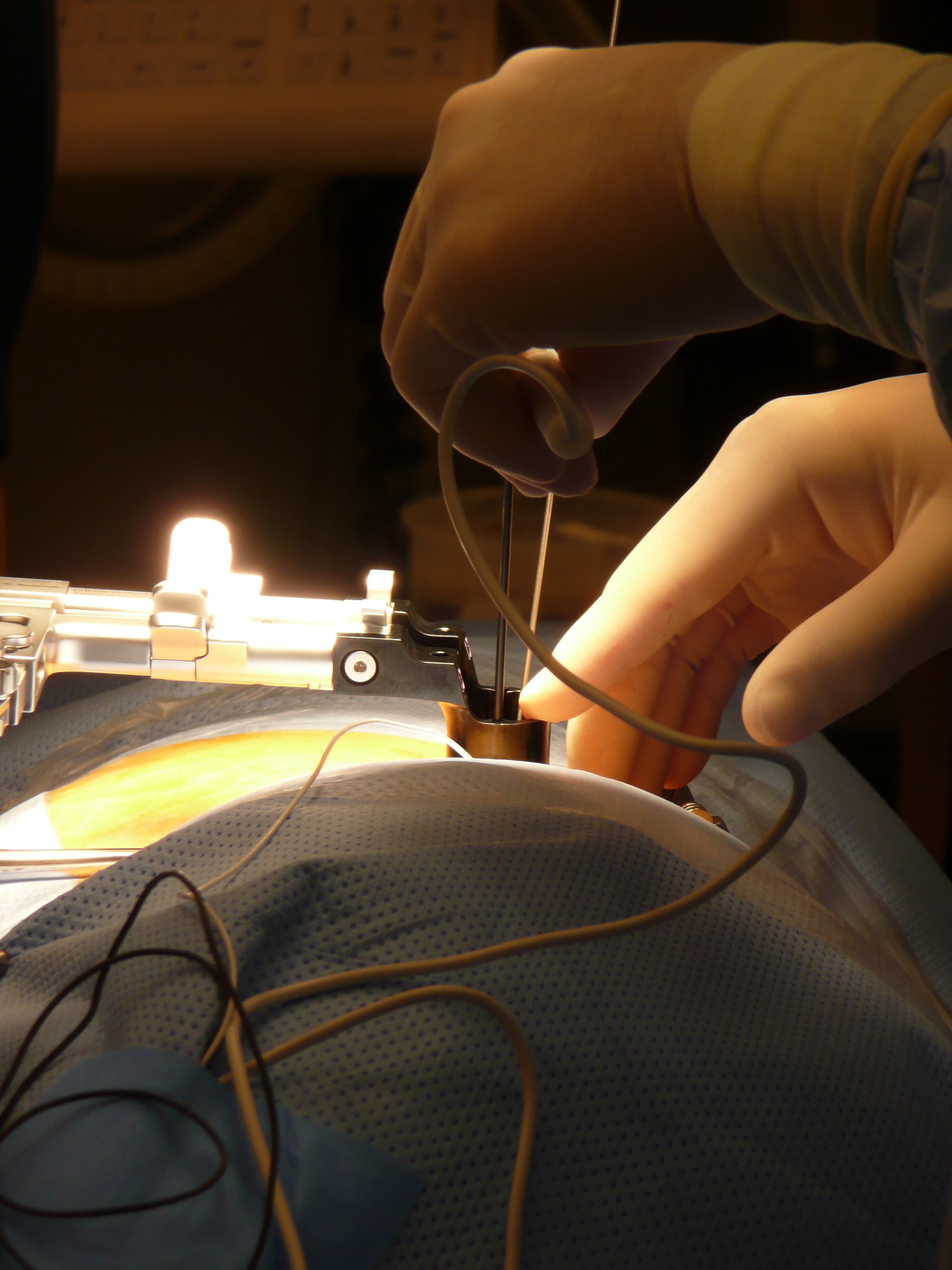
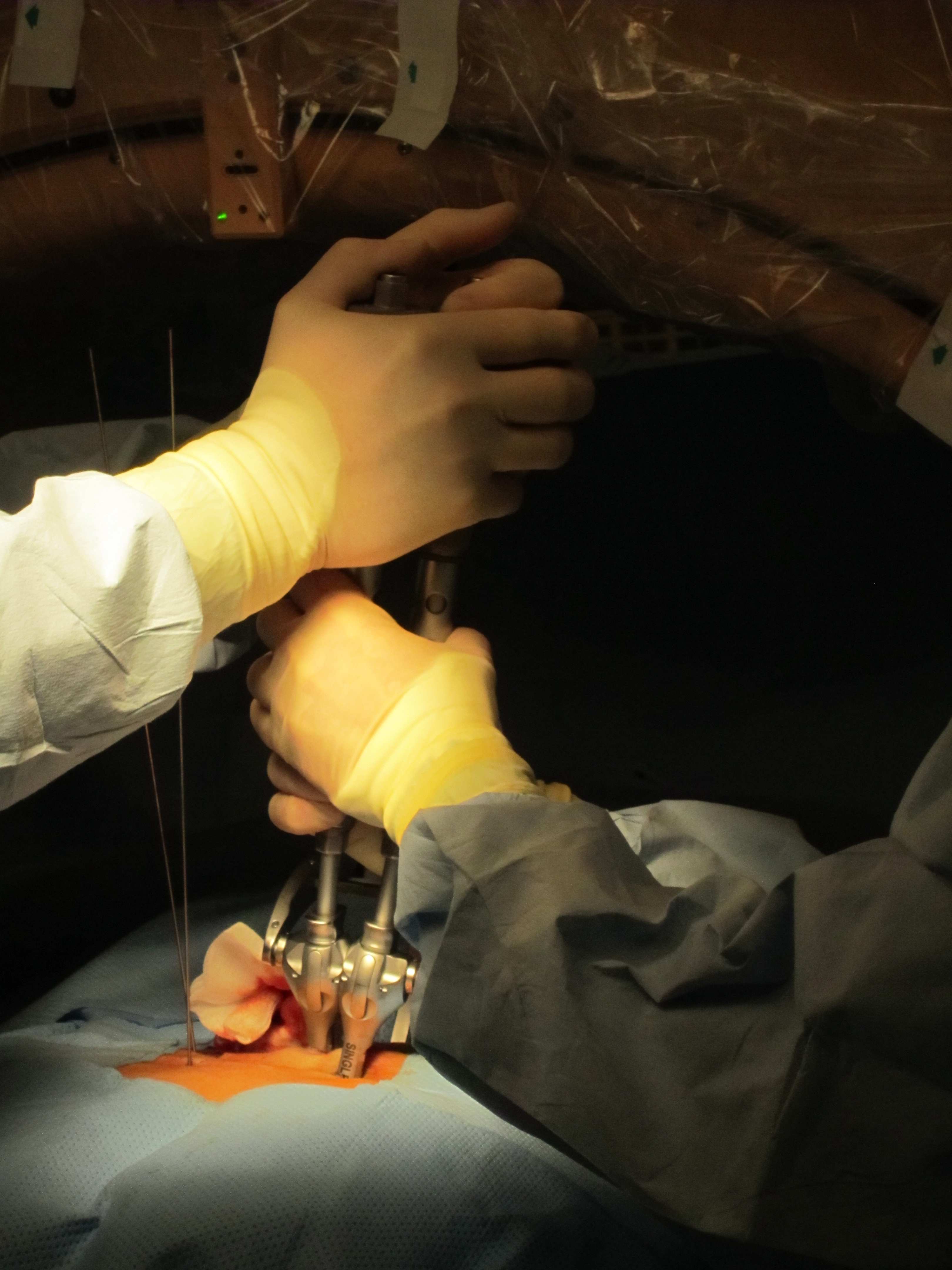
In addition to the complete practice of general spine and brain neurosurgery, Dr. Schils offers tailored solutions to all surgical spine problems by using innovative, elegant and less invasive options (O-Arm, Neuro-navigation, Microscopes, new surgical techniques). These encompass all cervical, thoracic and lumbar pathologies. Dr. Schils has developed an expertise in minimally invasive neurosurgery, in new approaches to the anterior and lateral spine, and in micro-invasive treatments for spinal fractures.
With respect to this, he is known in the scientific community and within the medical industry. Medical companies regularly request his services for the elaboration of new medical techniques and solutions.
In the margin, an overview of the most frequently observed problems.
SPINE SURGERY
Cervical spine
The common denominator of surgical solutions is to remove compression on the nerve endings or on the spinal cord that is responsible for pain or neurologic signs.
The source of compression can be a spinal herniated disc, an osteophyte (arthrosis, foraminal stenosis, a reduced or stenotic cervical canal), a calcification of the ligaments or even a bone fracture, an abscess (an infected lesion) or a tumor.
The most frequent initial symptoms are pain (in the cervical spine or radiating in the arm, cervico-brachialgia, cervico-brachial nevralgia, torticolis), paresthesia (the sensation of tingling, tickling, pricking, or burning of a person’s skin) and the partial or complete loss of motricity (paresis, paralysis). The aim of decompression is to eliminate the pain or neurologic symptoms and to potentially permit recuperation of the nerve lesion or of the spinal cord by guaranteeing the stability of the spine after an operation which can lead to a return to social, professional and leisure activities.
The time needed for convalescence and the delay required to return to normal activities depends on the type of pathology, the surgical technique used and the specifics of each patient. In all cases, a personalized agenda for progressively undertaking different activities will be proposed.
- Cervical disc herniation
- Cervico-arthrosic medullopathy
- Cervical arthrosis, foramen stenosis
- Trauma and tumors
Either via an anterior approach with fusion, or via an anterior approach using a disc prosthesis in order to preserve mobility, or via a posterior approach. Rapid recovery (2-6 weeks), return home within 2-3 days, no neck brace, post-surgical physiotherapy recommended.
Stenotic or reduced cervical canal, anterior and/or posterior approach with decompression (discectomy or corpectomy) and fusion.
Anterior approach, decompression and fusion.
Fractures of the spine, instability, primary tumors or bone metastases.
Thoracic spine
- Thoracic disc herniation, tumors or fractures.
Lumbar spine
- Lumbar disc herniation
- Foraminal and extra-foraminal disc herniations
- Narrow lumbar canal / lumbar stenosis
- Fractures
- Lumbar Discopathies
Microdiscectomy, micro-decompression. The symptoms are back pain or radiation in the legs (lumbago, sciatica) sometimes associated with paresthesia (the sensation of tingling, tickling, pricking, or burning of a person’s skin) or a motor deficit (loss of motricity in the leg or foot). The microscopy technique permits the removal of pieces of the disc that are in contact with a nerve and preserves all the muscle, bone and ligament structures. There is no loss of mobility after the surgery, the stay in the clinic is between 3-4 days, and the return to professional activity in generally within 3-4 weeks. As soon as you return home, physiotherapy can begin.
Laminectomy and selective micro-decompression. An extremely frequent situation where progressive compression of the lumbar nerve roots occur in the spinal canal following wear on different spinal structures (intervertebral discs, ligaments, articulations). The symptoms can be either back or leg pain, an intolerance to prolonged standing, walking difficulties (neurogenic claudication), paresthesia or problems with motricity. The aim of the intervention is to make space for the nerve structures, thus permitting a rapid, important and durable improvement of the symptoms.
Traumatic, osteoporotic or tumor fractures (Kyphoplasty, Kivaplasty, Vertebroplasty), percutaneous fixation. Recently new techniques permit the treatment of these problems using skin micro-incisions and by single injection in the vertebra of biological cement.
Progressive wear of the disc (disc degeneration) is responsible for chronic pain in the lower back, lumbago, the loss of lumbar comfort or a reduction in quality of life.
Possible techniques (every indication is the result of a detailed study of your clinical situation and your radiology file):
- ALIF: Anterior Lumbar Interbody Fusion
- TDR: Artificial Disc,Total Disc Remplacement
- XLIF: Extreme Lateral Interbody Fusion
- Lumbar Decompressions and Instrumentations
- PLIF: Posterior Lumbar Interbody Fusion
- TLIF: Transforaminal Interbody Fusion
- MISS: Minimally Invasive Spine Surgery
- Complex spine: revision spine surgery – degenerative scoliosis
SPINE SURGERY
Cervical spine
The common denominator of surgical solutions is to remove compression on the nerve endings or on the spinal cord that is responsible for pain or neurologic signs.
The source of compression can be a spinal herniated disc, an osteophyte (arthrosis, foraminal stenosis, a reduced or stenotic cervical canal), a calcification of the ligaments or even a bone fracture, an abscess (an infected lesion) or a tumor.
The most frequent initial symptoms are pain (in the cervical spine or radiating in the arm, cervico-brachialgia, cervico-brachial nevralgia, torticolis), paresthesia (the sensation of tingling, tickling, pricking, or burning of a person’s skin) and the partial or complete loss of motricity (paresis, paralysis). The aim of decompression is to eliminate the pain or neurologic symptoms and to potentially permit recuperation of the nerve lesion or of the spinal cord by guaranteeing the stability of the spine after an operation which can lead to a return to social, professional and leisure activities.
The time needed for convalescence and the delay required to return to normal activities depends on the type of pathology, the surgical technique used and the specifics of each patient. In all cases, a personalized agenda for progressively undertaking different activities will be proposed.
- Cervical disc herniation
- Cervico-arthrosic medullopathy
- Cervical arthrosis, foraminal stenosis
- Trauma and tumors
Either via an anterior approach with fusion, or via an anterior approach using a disc prosthesis in order to preserve mobility, or via a posterior approach. Rapid recovery (2-6 weeks), return home within 2-3 days, no neck brace, post-surgical physiotherapy recommended.
Stenotic or reduced cervical canal, anterior and/or posterior approach with decompression (discectomy or corpectomy) and fusion.
Anterior approach, decompression and fusion.
Fractures of the spine, instability, primary tumors or bone metastases.
SPINE SURGERY
Thoracic spine
Thoracic disc herniation, tumors or fractures.
SPINE SURGERY
Lumbar spine
- Lumbar disc herniation
- Foraminal and extra-foraminal disc herniations
- Narrow lumbar canal / lumbar stenosis
- Fractures
- Lumbar Discopathies
Microdiscectomy, micro-decompression. The symptoms are back pain or radiation in the legs (lumbago, sciatica) sometimes associated with paresthesia (the sensation of tingling, tickling, pricking, or burning of a person’s skin) or a motor deficit (loss of motricity in the leg or foot). The microscopy technique permits the removal of pieces of the disc that are in contact with a nerve and preserves all the muscle, bone and ligament structures. There is no loss of mobility after the surgery, the stay in the clinic is between 3-4 days, and the return to professional activity in generally within 3-4 weeks. As soon as you return home, physiotherapy can begin.
Laminectomy and selective micro-decompression. An extremely frequent situation where progressive compression of the lumbar nerve roots occur in the spinal canal following wear on different spinal structures (intervertebral discs, ligaments, articulations). The symptoms can be either back or leg pain, an intolerance to prolonged standing, walking difficulties (neurogenic claudication), paresthesia or problems with motricity. The aim of the intervention is to make space for the nerve structures, thus permitting a rapid, important and durable improvement of the symptoms.
Traumatic, osteoporotic or tumor fractures (Kyphoplasty, Kivaplasty, Vertebroplasty), percutaneous fixation. Recently new techniques permit the treatment of these problems using skin micro-incisions and by single injection in the vertebra of biological cement.
Progressive wear of the disc (disc degeneration) is responsible for chronic pain in the lower back, lumbago, the loss of lumbar comfort or a reduction in quality of life.
Possible techniques (every indication is the result of a detailed study of your clinical situation and your radiology file):
- ALIF: Anterior Lumbar Interbody Fusion
- TDR: Artificial Disc,Total Disc Remplacement
- XLIF: Extreme Lateral Interbody Fusion
- Lumbar Decompressions and Instrumentations
- PLIF: Posterior Lumbar Interbody Fusion
- TLIF: Transforaminal Interbody Fusion
- MISS: Minimally Invasive Spine Surgery
- Complex spine: revision spine surgery – degenerative scoliosis
BRAIN SURGERY
Interventions for tumors
Benign or malignant tumors, meningiomas, gliomas, bone tumors of the skull, cerebral metastases; using neuro-navigation techniques.
After a complete surgical work-up, the lesion can be removed by opening the skull (craniotomy) and by using neuro-navigation. All interventions can be programmed and followed in real time on a computer thus increasing the surgical precision. This can be compared to an ultra-performance GPS. Any resected lesion is systematically sent to the laboratory in order to establish the diagnosis with certainty according to the nature of the process.
Intervention for hydrocephaly
Ventriculo-peritoneal derivation / shunt
This is a benign intervention that requires only 2-3 days in the clinic and slows down the evolution of the symptoms. All follow-up concerning the fine-tuning of the valve can secondarily be performed on an out-patient basis.
Cerebral biopsy
Evacuation of hematomas (sub-dural, intra-cerebral)
BRAIN SURGERY
Interventions for tumors
Benign or malignant tumors, meningiomas, gliomas, bone tumors of the skull, cerebral metastases; using neuro-navigation techniques.
After a complete surgical work-up, the lesion can be removed by opening the skull (craniotomy) and by using neuro-navigation. All interventions can be programmed and followed in real time on a computer thus increasing the surgical precision. This can be compared to an ultra-performance GPS. Any resected lesion is systematically sent to the laboratory in order to establish the diagnosis with certainty according to the nature of the process.
BRAIN SURGERY
Intervention for hydrocephaly
Ventriculo-peritoneal derivation / shunt
This is a benign intervention that requires only 2-3 days in the clinic and slows down the evolution of the symptoms. All follow-up concerning the fine-tuning of the valve can secondarily be performed on an out-patient basis.
BRAIN SURGERY
Cerebral biopsy
BRAIN SURGERY
Evacuation of hematomas (sub-dural, intra-cerebral)
NEUROSURGERY FOR PAIN
Posterior spinal cord neurostimulation
also at high frequency
Chronic back pain can appear either in patients who already underwent surgery and are still in pain or in patients for whom no therapeutic etiologic intervention is possible. When classical treatment (medication, infiltration, manual therapy, etc.) has been tried without success and when the impact on quality of life becomes significant, a surgical treatment of the pain symptoms can be considered. In well selected patients, small electrodes can be placed by a neurosurgeon in contact with the spinal cord and can mask the pain signal that goes to the brain (a system that can be slightly compared to a Pacemaker). These treatments require a multi-disciplinary evaluation and follow-up but within the last few years have known a substantial development.
PLAGIOCEPHALY
Our present lifestyles (Maxi-cosy, car seats, active and mobile parents), in addition to the evolution in medicine (the recommendation to lay children on their back in order to avoid sudden death syndrome) lead to an increased frequency of babies with flat heads (phagiocephaly). Often the medical community gives a reassuring message to parents of its systematic spontaneous correction. However, certain severe forms or late diagnosis can lead to resistance with respect to classical treatment (kinesitherapy, osteopath, changing of position) and a treatment by dynamic cranial orthesis must be considered. Our team (neurosurgeon, ergotherapist, osteopath and kinesitherapist) is specialized since 10 years in the treatment of this frequent problem which often causes parental anxiety.



Contacts and Additional Information
The treatment protocol comprises a diagnostic consultation, a phase where the orthesis is created and a follow-up period.
The consultation and the follow-up examinations are performed in Belgium and Switzerland.
The phase for creating the orthesis is currently done only in Belgium (2 required consultations).
For appointments:
By telephone: +32-472-80.81.32
By e-mail: plagiodocteurschils@gmail.com
Plagiocephaly office:
Dr Schils- Mmes Jehaes et Bradfer
Rue Libon 5
4800 Verviers
Belgium
The Geneva private clinics have continually invested money in order to offer the most modern and high performance array of technical apparatus in the operating room, thus permitting to practice neurosurgery, and in particular, back surgery. All clinics where Dr. Schils works have the most recent neurosurgical microscopes, neuro-navigation systems, O-Arm (intra-operative CT) or neuro-monitoring which permit the best actual conditions of security and precision. Dr. Schils has several years of experience with these different techniques and he publishes regularly concerning the potential advantages of these surgical tools. In addition to the advanced technical apparatus in the operating room, the clinics have both a floor-bound and operating room nursing staff that is extremely well-trained and competent, offering the patient, in addition to the surgical expertise, optimal health-care conditions and an ear for listening during the patient’s stay. Dr. Schils has invested much time in a multi-disciplinary collaboration between himself and his colleagues in the departments of radiology, physiotherapy, molecular imagery, anti-ageing, anesthesiology, neurology, rheumatology, oncology, etc. This guarantees that the patient has an integrated, optimized and continuous approach. Finally the clinics guarantee a stay with a personalized welcome, maximum comfort and comparable luxury hotel services. In addition, a private porter service is available 24 hours a day.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

Switzerland, and especially Geneva, have a well-known international reputation for service, excellence and precision, mandatory qualities for the practice of neurosurgery. With respect to his training, Dr. Schils quickly developed his international activities by perfecting his expertise in foreign countries and by teaching and helping surgeons around the world who later became his friends. At present, and due to the exceptional welcome at the private Geneva clinics, he can offer treatment options to patients from around the world. His passionate research for the best treatment options for his patient insures an increasing demand from international patients. His services can include a simple medical opinion concerning a patient’s file to a surgical intervention in Geneva, and/or an office visit in Geneva or in the patient’s own country, his surgical assistance in the patient’s country or the recommendation of a colleague in the patient’s country. A personalized service of accompaniment is frequently put in place during your medical stay in Geneva. Due to this service, even the most specific requests can be met within the shortest time. After an initial contact with Dr. Schils, he will direct you towards his secretarial personnel who will answer all of your administrative requests and requirements (insurance questions, cost quote calculation, establishing the medical program, organization of your travel and lodging). All requests for advice are associated with the greatest discretion and the highest professionalism. A summary of your consultation and the advice provided to you will be given to you either in French or English after your visit. Other languages are available depending on the delay and the specific conditions.
- Physio Conference Geneva: "Minimally invasive approaches to spine surgery", Geneva, Switzerland, May 23, 2014
- Physio Conference at Clinique Générale-Beaulieu: « Updates on spines surgery », February 5th 2015, Geneva, Switzerland
- Conference UNO: « Latest developments in treatments and prevention of back pain problems. », February 26th 2015, Geneva, Switzerland
- SFCR (French Society of Spine Surgery): Annual meeting, Paris, June 5-7, 2014
- SOLAS (Society of Lateral Access to the Spine): EMEA meeting, Italy, Nov 18-19, 2014
- EUROSPINE: Annual meeting, Lyon, France, Oct 1-3, 20-14
- XLIF Meeting, October 27, 2014, Bern, Switzerland (Chairman)
- Training Sales Experts, November 19, 2014, Tolochenaz, Switzerland (Faculty)
- BKP Course, December 4-5 2014, Leiden, The Netherlands (Faculty)
- Proctoring vertebral fracture treatment with the KIVA System (Zimmer), Sion, Valais, Switzerland, September 2, 2014
- Live Surgery with 20 Chinese neurosurgeons, specialists in spinal surgery: Lateral approach to the spine (Nuvasive), Clinique Générale Beaulieu, Geneva, Switzerland, June 24, 2014
- Surgeon to surgeon proctoring program: Lateral approach to the spine (Medtronic), Amman, Jordan, March 17-20, 2014
Advertising campaign – Clinique Générale-Beaulieu

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
12, Chemin Beau-Soleil, 1206 Genève, Suisse
Tel : +41 22 329 45 20
Fax : +41 22 329 47 14
Email : info@schilsneurosurgery.com
Dr. Schils’s entire team is available for any information request or meeting appointment.
Office hours :
Monday, Tuesday, Thursday, Friday from 9:00 AM to 5:00 PM
Wednesday from 9:00 AM to 12:00 AM
Dr. Schils can be contacted at any time outside the above-mentioned office hours by directly contacting the clinics.
Practical information:
During your visit to Dr. Schils, please remember to take your most recent radiological pictures/documents, your medication list and a short summary of your medical history.
Public transports :
– By bus: — bus line #3 or #21 — stop « Crêts-de-Champel »
– From Geneva International airport (Cointrin) — 20 minutes trip
– Cornavin train station (Geneva center) — 10 minutes trip